
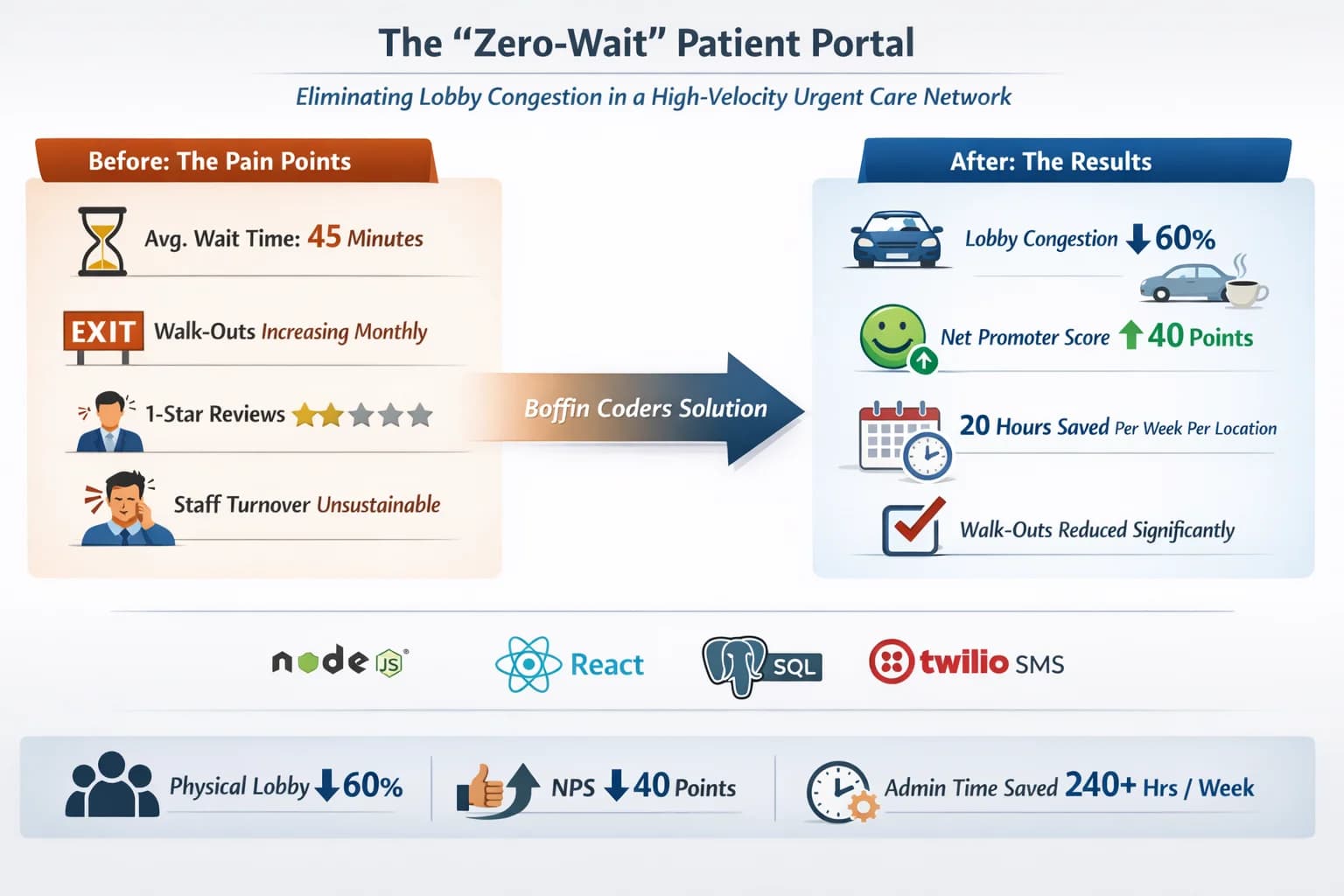
Key Outcomes
60%
Lobby Congestion Reduction
+40 Points
Net Promoter Score Increase
Technologies Used
1. Executive Summary
A rapidly expanding urgent care franchise was losing patients before care even began.
Across 12 high-traffic locations handling 15,000 monthly visits, the organization was bleeding patient trust — not because of poor clinical outcomes, but because of perceived chaos in the waiting experience.
Key symptoms:
- Average wait time: 45 minutes
- Walk-outs: Increasing monthly
- 1-Star Google Reviews: Escalating
- Front-Desk Staff Turnover: Unsustainable
Leadership initially believed they had a staffing problem.
They did not.
They had a queue transparency failure.
Boffin Coders was brought in not to “build a portal,” but to answer a deeper strategic question:
How do we eliminate lobby congestion without hiring more staff or expanding square footage?
After a structured diagnostic phase, we designed a real-time digital queuing architecture using Node.js (WebSockets), React dashboards, PostgreSQL, and Twilio SMS.
The system ultimately:
- Reduced physical lobby congestion by 60%
- Improved Net Promoter Score by 40 points
- Saved 20 hours per week per location in administrative overhead
This case study is not about software features.
It is about diagnosing operational friction — and redesigning flow at scale.
The Client Context: Why Failure Was Not an Option
This was not a startup experimenting with innovation.
It was a fast-growing urgent care franchise operating 12 high-traffic locations, competing aggressively on speed and accessibility.
The Operating Reality
- 15,000 patient visits per month
- Peak traffic: 5:00 PM – 8:00 PM
- Pediatric, trauma, and urgent cases mixed in one physical queue
- Walk-in dominant model
The front desk had become the single bottleneck responsible for:
- Check-in
- Insurance capture
- Wait time communication
- Patient status updates
- Complaint handling
The brand promise was speed.
Instead, speed became its vulnerability.
The Compounding Risk
Healthcare is emotionally charged.
A 45-minute wait does not feel like 45 minutes when:
- A child has a fever
- A patient is bleeding
- Someone left work early for urgent treatment
Every minute without communication multiplies anxiety.
Anxiety turns into:
- Walk-outs
- Refund demands
- 1-star Google Reviews
- Social media escalation
- Brand erosion
Leadership was explicit:
“We cannot afford another quarter of 1-star reviews.”
This was not a technical inconvenience.
It was reputational risk at scale.
The Diagnostic Phase: Finding the Real Problem
At Boffin Coders, we do not begin with technology.
We begin with systems thinking.
Before writing a single line of code, we ran a structured audit across business, operations, and technology.
What We Observed on the Surface
Symptoms were obvious:
- Overcrowded waiting rooms
- Patients repeatedly approaching the front desk
- Staff manually calling out names
- No real-time visibility into queue progress
Most vendors would immediately suggest:
“You need online check-in.”
That would have been a mistake.
What We Actually Audited
1. Operational Flow
Patient arrival → intake → triage → provider assignment

We analyzed variability by:
- Location
- Time of day
- Staffing mix
2. Human Behavior
We measured:
- How often patients asked for updates
- How staff responded under pressure
- Where emotional trust broke down
3. Data & Systems
We examined:
- What timestamps existed
- What real-time status signals did not
- How disconnected systems forced manual updates
4. Front Desk Reality
Front-desk staff were not inefficient.
They were functioning as a human message bus.
Every queue update flowed through them.
The Root Cause
The real issue was not wait time.
It was uncertainty.
Patients were willing to wait 30–45 minutes — if they understood:
- Where they were in line
- How long it would realistically take
- When they actually needed to be physically present
Instead, the system forced:
- Patients to occupy physical space
- Staff to repeat the same explanations
- Leadership to absorb reputational damage
Technically speaking, the system lacked real-time state synchronization between:
- Patient
- Front desk
- Clinical operations
Everything else cascaded from that architectural gap.
The Insight That Changed Strategy
Once we reframed the problem correctly, the solution space shifted.
This was not a staffing issue. It was not a scheduling issue.
It was a real-time communication issue.
The opportunity became clear:
- Decouple waiting from physical presence
- Replace human polling with system-driven updates
- Turn uncertainty into predictability
Only then did technology enter the discussion.
Risk Assessment Before Prescribing Code
Before proposing architecture, we evaluated constraints:
Constraint 1 — Healthcare Compliance
No sensitive PHI over SMS or public dashboards.
Constraint 2 — Existing EHR Integration
We could not replace the core electronic health record.
Constraint 3 — Non-Technical Staff
UX had to be frictionless.
Constraint 4 — Multi-Location Scalability
12 locations now. 20+ projected within 24 months.
Constraint 5 — Peak Load
Simultaneous updates across all locations during evening rush.
This was not a brochure site.
It was a mission-critical operational system.
THE ARCHITECTURE
Designing for Flow, Not Features
Once the true issue — uncertainty at scale — was isolated, the objective changed.
We were not reducing wait times.
We were redesigning flow.
Three non-negotiable principles guided the strategy:
- Decouple presence from progress: Patients should not need to sit in a lobby to hold their place.
- Make the system speak first: Staff should not be the primary source of updates.
- Design for peak chaos, not average calm: The system must work during flu season, not just quiet mornings.
Why This Technology Stack
Every technology decision supported real-time state and reliability.
Node.js — The Real-Time Core
We needed:
- Thousands of concurrent connections
- Instant updates
- Predictable performance under bursts
Node.js’ event-driven, non-blocking architecture made it ideal for:
- WebSocket-based updates
- High I/O workloads
- Stateful connection management
We did not build APIs that patients poll.
We built systems that notify.
React — Interface as State
The front desk and dashboards required:
- Immediate visual updates
- Zero-refresh mental models
- Reduced cognitive load
React allowed the UI to behave as a function of state.
When a patient moved from:
“Checked In” → “In Triage” → “Next Up”
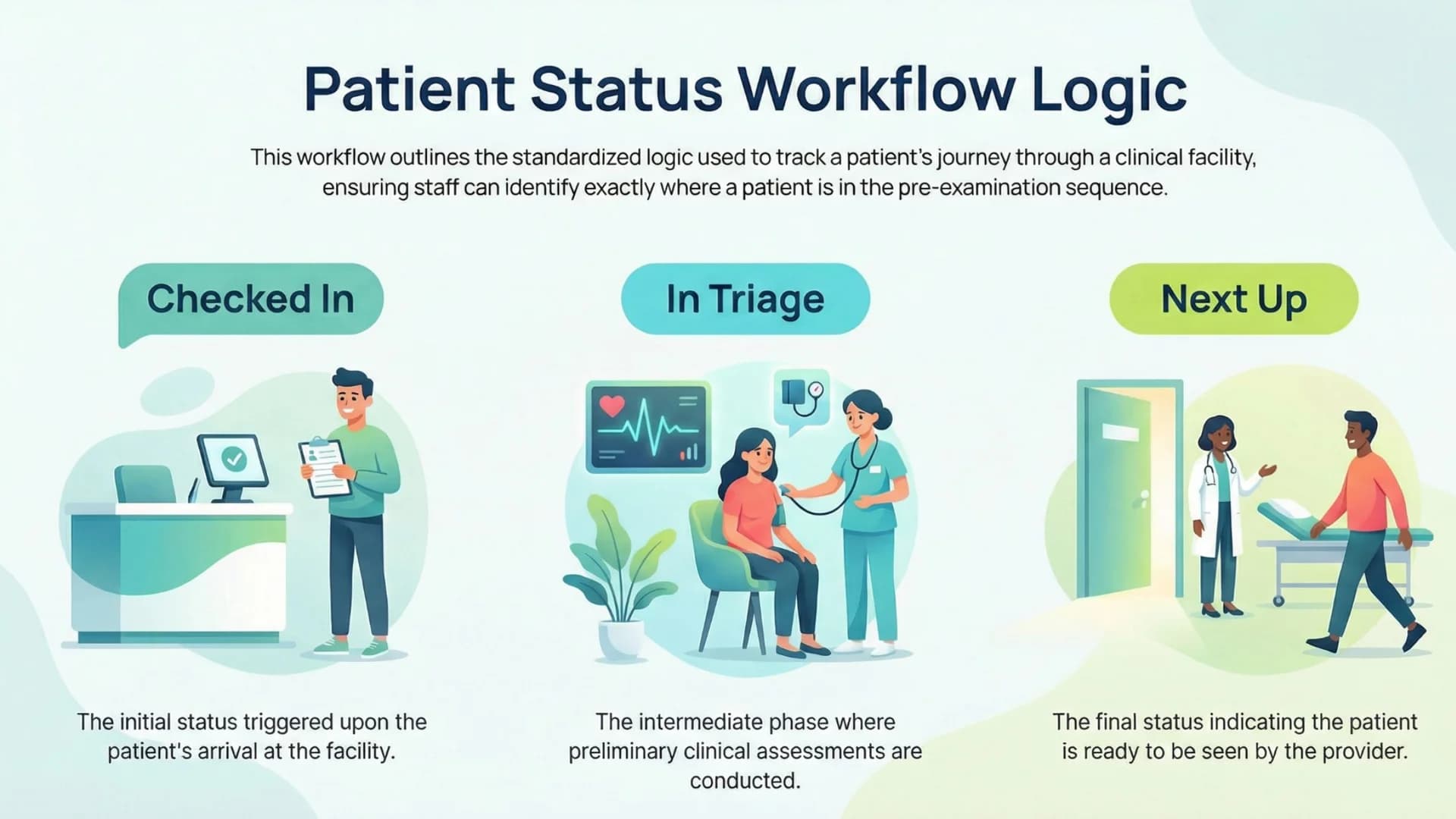
…the interface re-rendered reality automatically.
Training time decreased.
Error rates fell.
PostgreSQL — The Source of Truth
Healthcare demands consistency.
PostgreSQL provided:
- ACID-compliant transactions
- Clear audit trails
- Reliable concurrency handling
Real-time systems still require a stable anchor.
PostgreSQL was that anchor.
Twilio — Meeting Patients Where They Are
SMS was not optional.
It was the primary patient interface.
Twilio ensured:
- High delivery reliability
- Compliance safeguards
- Scalable APIs
No apps to install.No friction.No learning curve.
How Data Actually Flows
At its core, the architecture operates as a closed feedback loop.
- Patient checks in (on-site or remotely).
- Visit record is created in PostgreSQL.
- Node.js maintains an active in-memory visit state.
- State changes emit WebSocket events.
- Dashboards update instantly.
- Triggered state transitions send SMS alerts.
Front desk updates once.
The system propagates everywhere.
No polling.No duplication.No human relay.
This eliminated congestion — not faster doctors, but faster truth.
Implementation Challenges
Trusting the System
Staff were accustomed to:
- Calling names manually
- Managing mental queues
- Answering repeated questions
We deployed gradually:
- Parallel runs during low-risk hours
- Manual override safeguards
- Visual confirmations matching reality
Trust was earned — not forced.
Real-Time Accuracy Under Chaos
Urgent care is unpredictable.
- Idempotent state transitions
- Guardrails against invalid jumps
- Role-based state ownership
Small inaccuracies destroy confidence quickly.
We engineered against them.
Scaling Beyond 12 Locations
The system was built for 50 locations from day one.
- Stateless services where possible
- Centralized configuration
- Location isolation namespaces
Adding a new clinic became configuration — not development.
THE ROI & FUTURE
Business Impact Within 90 Days
1. Lobby Congestion ↓ 60%
Before:
- 18–25 patients in peak-hour lobbies
- Standing-room frustration
After:
- Patients waiting in cars
- Nearby cafés
- Outdoor spaces
The lobby became a transition space — not a holding tank.
2. Net Promoter Score ↑ 40 Points
Clinical quality did not change.
Transparency did.
Patients felt:
- Informed
- In control
- Respected
In healthcare, perceived respect is currency.
3. Administrative Time Saved
20 hours per week per location.
Across 12 locations:
- 240 hours weekly
- 12,480 hours annually
At $20/hour: ≈ $250,000 annual efficiency unlocked.
Without hiring.
4. Walk-Out Reduction
Even a 5% drop in walk-outs at 15,000 monthly visits represents significant revenue recovery.
Small friction reductions scale aggressively in healthcare.
5. Staff Morale Improvement
The system removed:
- Repetitive interruptions
- Emotional confrontations
- Queue anxiety
Staff feedback:
“It feels calmer.” “We’re not constantly defending wait times.”
Technology reduced cognitive load.
Financial Framing
Metric | Annual Impact |
Admin Efficiency | ~$250K |
Reduced Walk-Outs | Variable but significant |
Brand Improvement | Long-term compound value |
Staff Retention | Hiring cost savings |
The system paid for itself rapidly.
Because it solved the root cause.
Future Outlook: 5-Year Scalability
This was never designed for 12 locations.
It was designed for 50.
Built-In Scalability
- Logical isolation per location
- Stateless front-end clients
- Event-driven extensibility
Next Evolution
With queue state digitized, future enhancements become possible:
- AI-based wait predictions
- Intelligent triage prioritization
- Automated staffing suggestions
- Predictive peak load alerts
- Executive real-time capacity dashboards
The system evolved from tool to data asset.
Strategic Lessons
- Operational pain is often architectural.
- Transparency outperforms marginal speed gains.
- Real-time systems create competitive advantage
Closing Reflection
The Zero-Wait Patient Portal was never just about building a digital portal — it was about eliminating uncertainty across the entire patient journey. Instead of focusing on surface-level features, we addressed the core problem: lack of transparency in high-demand environments. As a result, we transformed key operational challenges into measurable improvements.
We transformed:
- A crowded lobby
- An overwhelmed front desk
- Escalating negative reviews
Into:
- A distributed, real-time queue intelligence system
- A calmer and more informed patient experience
- A scalable operational backbone designed for growth
Technology, when implemented with the right strategy, should remove friction rather than add complexity. When designed correctly, it becomes invisible to the user — yet invaluable to the organization.
Ready to Build Something
That Actually Works?
Stop patching legacy code. Let's engineer a platform that scales with your ambition.